BMI
Patients who snore are commonly overweight, and one
of the first lines of management is to encourage patients
to attain the ideal weight for their height. A simple
method of determining the ideal weight is by calculating
the Body Mass Index (BMI). This is done by dividing the
weight in Kg by the height in metres, squared.
ie. weight (Kg) / height * height (m)
A BMI greater than 25 is considered overweight and the
patient would benefit from diet and exercise.
Epworth
Patients with significant obstructive sleep
apnoea syndrome are usually excessively tired during the
day. They fall asleep easily during mundane activities
and this is assessed by a simple
questionnaire which gives a result known as the
Epworth score. Epworth scores of 16 and above are
suggestive of significant OSA and warrant more detailed
investigation such as an overnight sleep study. This is
obviously a rough guide and occasionally patients have a
low Epworth score despite having OSA.
Alcohol
Alcohol causes relaxation of the pharyngeal
muscles and therefore they tend to collapse and narrow
the pharyngeal lumen cross-sectional area. This is
particularly enhanced during deep sleep and increases the
tendency to snore. It is suggested that snorers should
avoid alcohol after 7pm.
Drugs
Sedative drugs have the same effect as alcohol in that
they precipitate relaxation of the pharyngeal muscles.
Sedative drugs such as 'sleeping tablets' or
antidepressants should be used at the minimum effective
dose under the supervision of the patient's General
Practitioner.
Nasal airway
The first point of narrowing of the upper
airway is the nasal airway. If the nose is blocked then
the patient makes increased effort to breathe in (inspiration).
Eventually the patient may breathe with the mouth partly
open and this increases the chance of snoring. Also the
increased effort of inspiration results in negative
pressure in the pharynx which leads to inwards collapse
of the loose membranes at the back of the throat and
precipitates snoring.
For these reasons it is important to ensure that the
nasal airway is excellent. Assessment of the nasal airway
by an ENT surgeon is important to check for such factors
as a deviated nasal septum , enlarged turbinates, nasal
polyps or even adenoids.
Pharynx
Examination of the throat may show a persistent narrowing
of the airway at the back of the mouth (oropharynx). This
is commonly due to enlarged tonsils or enlargement (hypertrophy)
of the lymphoid tissue at the back of the tongue.  Sometimes there is a broad flap
of mucosal membrane hanging down from the edge of the
soft palate. These anatomical factors often need to be
corrected in order to maximise the upper airway during
sleep and reduce snoring.
Sometimes there is a broad flap
of mucosal membrane hanging down from the edge of the
soft palate. These anatomical factors often need to be
corrected in order to maximise the upper airway during
sleep and reduce snoring.
Tape recording
It is useful to have proof that the patient
actually has a true snoring problem before embarking on a
course of treatment. Sometimes the "snoring noise"
which disturbs one person is assessed as merely light
breathing by others and would not justify invasive
surgery! Also a genuinely disruptive noise may be due to
expiratory grunting (noise while breathing out) rather
than the commoner inspiratory (breathing in) rattling
snore noise. An easy way of checking this is to make a
tape recording of the snoring noise. Ideally the partner
should video the snorer with a simple camcorder. An
alternative is to use a simple dictaphone recorder or
radiocassette recorder. Ten minutes of representative
snoring is sufficient to give the doctor a good
impression of the type and severity of the snoring
problem. This simple test does not replace a full
overnight sleep study (see below) in cases of suspected
severe Obstructive Sleep Apnoea but gives useful
information in mild cases and simple snoring when the
expense and inconvenience of a formal sleep study is not
justified.
Overnight sleep study (Polysomnography)
If significant OSA is suspected then the
patient will require a full ovenight sleep study. This
may be carried out in hospital in a specialist sleep
laboratory or the patient may be fitted with recording
equipment and allowed to sleep at home.
In most cases the patient is connected to a range of
monitoring devices for the whole night. The results are
then recorded in a computer programme and analysed to
look for evidence of OSA.
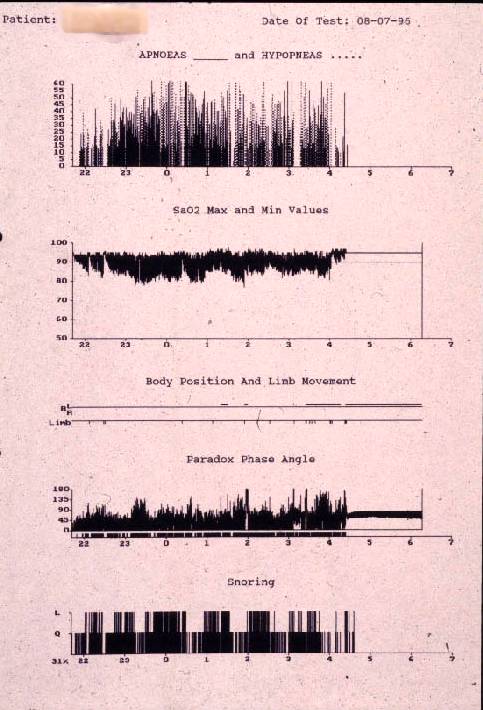 Typical measurements
include heart rate, nostril airflow, chest wall movement
and oxygen concentration of the blood. Some systems
determine the type of electrical brain activity during
sleep (EEG) and can indicate the stage of sleep. Some
systems monitor pressure inside the gullet and give an
indication of obstructed breathing when the pressure is
excessively negative.
Typical measurements
include heart rate, nostril airflow, chest wall movement
and oxygen concentration of the blood. Some systems
determine the type of electrical brain activity during
sleep (EEG) and can indicate the stage of sleep. Some
systems monitor pressure inside the gullet and give an
indication of obstructed breathing when the pressure is
excessively negative.